

Alcohol Consumption and Brain Health
Alcohol Consumption and Brain Health
How does alcohol affect our brains?

Hey Brainiacs,
Welcome to this week’s newsletter! It’s a hot topic this week; we’re going to talk about alcohol and the brain.
Alcohol and The Brain
Man, oh man, did this seem to get people fired up online! So, let’s get into it.
First and foremost, I am not telling anyone not to drink. I myself drink occasionally. What I am trying to tell people is that research suggests there are negative impacts of drinking on the brain, and we should be aware of this. I’m advocating for informed decision-making.
Secondly, research is nuanced, ever-changing, and complex. Methodologies need to be heavily scrutinized, and even then, we may not capture the full story. In the 1950’s physicians were often recommending patients to start smoking, and advertising suggested smoking was healthy1,2. Although we now know this isn’t the case – smoking increases the risk of heart disease, stroke, cancer, gum disease, cataracts, and much more – biased research and advertising suggested to the public otherwise. My point: we need to be cautious when reading studies; we should question if they show what they say they do and if they used the proper methods.
Finally, I don’t think there is conclusive, causative evidence to say just how bad alcohol is for your brain. More research needs to be done. However, I do think that the associative evidence that we have is compelling, as does the World Health Organisation3. They listed alcohol use as one of the top causes of disease burden back in 20093. And in 2017, an editorial published in the British Medical Journal provided an explanation for the conflicting evidence surrounding brain health effects and mild-to-moderate drinking, and ultimately concluded that as alcohol intake increases, so does the risk to our health, probably in a dose-dependent way4.
Correlation, Association, and Causation
Let’s get into some science terminology.
Correlation means that there is a linear trend between two factors. For example, ice cream sales increase when car sales increase. They’re correlated because they both increase.
Association means that one factor provides information about another factor. Based on the ice cream-car correlation, we know that if ice cream sales were rising, car sales were rising too. So, information about ice cream informs us about cars; this correlation is also an association.
However, correlation and association do NOT automatically mean there is causation. Causation means that without one factor, the other would not happen. If we stopped those ice cream sales, do we really think car sales would stop?
Causation is a lot trickier to show because you need to be able to manipulate the factors, which you often cannot do. We can't stop all ice cream shops from selling ice cream. We can’t stop all car dealerships from selling cars.
In terms of alcohol, you can’t force some people to drink a lot of alcohol and force others to drink none at all, and then look at their brains. This means we only have observational data, or data we get from observing people without intervening. This is problematic for causation because the reasons people do/don’t drink might affect other things in their life which will impact their brain health. For example, someone who doesn’t drink because they are worried about their health might exercise more, which will increase their brain volume. Someone who drinks socially but doesn’t exercise might have smaller brain volume just because they don’t exercise. So we need to make sure studies are accounting for these effects.
Alcohol and Brain Volume
Armed with our new knowledge, let’s look at some studies together. There are a lot more studies out there, but I’m going to present one which I referenced in a podcast recently, and one which seemingly shows an ‘opposite’ effect.
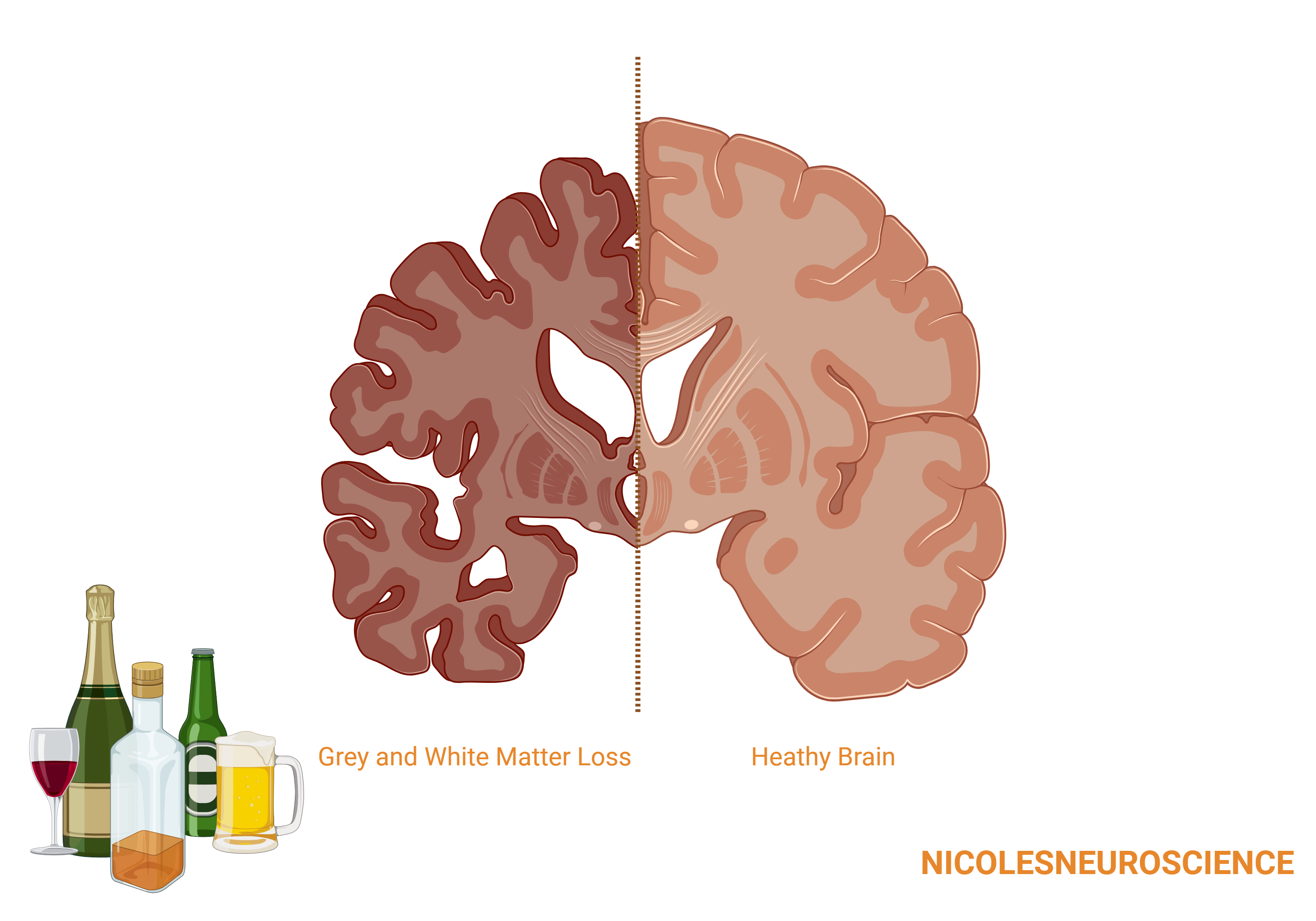
The paper I referenced found that alcohol intake is negatively associated with brain volume measures, in both grey and white matter5. This association was weak with people drinking 1 unit a day (although still present), moderate when people drank 2 units a day, and strong when people drank 3 units a day. (For reference, a standard glass of wine (175ml) is 2 units and a bottle of lager/beer/cider (330ml, ABV 5%) is 1.7 units). To illustrate what this association means, they quantified brain loss in terms of aging. Increasing from one daily unit of alcohol to two daily units of alcohol caused brain loss equivalent to 1.7 years of aging.

The researcher used data from 36,678 people; the people were all healthy, middle-aged or older, and living in the UK. The study controlled for age, height, handedness, sex, smoking status, socioeconomic status, genetic ancestry, and county of residence. Plus, they did an extended analysis controlling for BMI, educational attainment, and weight.
It’s a pretty robust study, albeit not perfect. There are better ways to control for the above variables, there are probably more variables that could have been controlled for, and the results cannot be generalized to people who are young, or not living in the UK. But, they show negative impacts of even one glass of wine a day on brain volume for a subset of the population.
Alcohol and Dementia
A paper which a lot of people brought up showed that maintaining mild to moderate drinking (2-4 units per day) or initiating mild (2 units or less per day) drinking was associated with a reduced risk of dementia6. A major limitation to highlight here is their outcome. Their outcome was a dementia diagnosis, however, the average age of included participants was 55, and on average, they were followed up for 6 years, but dementia cannot officially be diagnosed until someone is 65. Additionally, a diagnosis of dementia is only one way to measure brain health, and is affected greatly by genetics and prior medical history, which they did not control for.
Another limitation is how they define sustained drinking, initiating drinking, and reduced drinking. They define these based on two clinic visits and self-reported outcomes of drinking at each; if at the first visit they did drink, and at the second visit they didn’t, they were considered reducers. But, if they start drinking again after the second visit, there is no way to know. And, there is no way to know at what point between those two visits (which were two years apart) they stopped drinking. Finally, there is no way to know why they stopped drinking, and this might impact the risk of dementia too. Maybe they stopped drinking because they were having other health issues, which may affect their risk of dementia.
However, the researchers did account for age, sex, smoking status, exercise, area of residence and income, and still found that mild drinkers who sustained mild drinking during follow-up had 21% reduced risk of having dementia than non-drinkers who remained non-drinkers throughout follow-up. They only found a 7% decreased risk in dementia in people who start drinking mildly compared to those who don’t start drinking. Additionally, they found that heavy drinking increases the risk of dementia. The study proposes that alcohol has prosurvival and neuroprotective functions which may contribute to the beneficial effect mild alcohol consumption apparently has on dementia. However, this speculation requires more research7.
Suppose the findings from this study were to hold in a more robust setting. In that case, it is still important to note that the study was conducted on people living in Korea, who were 40 years or older and registered with the National Health Service, so these results apply to a specific population.
A Note on Blue Zones
When negative health impacts of alcohol consumption are brought up, someone always inevitably asks, “well, what about countries in the blue zone?” These regions include Italy, Greece and Japan, some of which are known partly for alcohol consumption. In these regions, people tend to live longer and healthier lives. However, major factors that influence their lengthened longevity include genetics, diet, lifestyle, and exercise. Genetics will differ in populations from different countries, and this will impact aging and how alcohol is metabolized. Diet and activity levels also vary greatly across countries, with the famed ‘Mediterranean diet’ being known for its positive health impacts. Another major factor is lifestyle and work-life balance, which is extremely variable across countries, and will impact stress levels which in turn can influence brain health. All of these factors - genetics, exercise, diet, stress - will impact the immune system, which also plays a critical role in brain health.
This is all to say that you cannot compare the effects of alcohol across different populations. It might be that alcohol impacts blue zones less (although it might not be that!) because they eat healthier, exercise more, have more robust immune systems, and are in a better position because of their genetics.
Important Updates
I will be going on a book tour in the US starting this week! So for the next two weeks, there will be no newsletter! Prepare yourselves to miss me.
The exciting news is that when I’m back from holiday, we’re going back to the basics on neurogenesis and neuroplasticity. I have noticed some confusion in the comments of my Instagram posts around these terms, so I am swooping in to clear that up.
I also have an exciting new member of the team to introduce when I’m back from holiday – so stay tuned!
Until next week,
Nicole x
References
https://tobacco.stanford.edu/
N. Oreskes, E. M. Conway, Merchants of Doubt: How a Handful of Scientists Obscured the Truth on Issues from Tobacco Smoke to Global Warming Bloomsbury Press, New York (2010).
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2800994
Holmes MV, Dale CE, Zuccolo L, et al. InterAct Consortium. Association between alcohol and cardiovascular disease: Mendelian randomisation analysis based on individual participant data. BMJ2014;357:g4164.