
Synaptic Plasticity
What is it and why do we need it?

Hey Brain Rewirers,
Welcome to this week’s newsletter! We’re going to do a deep dive into the mechanisms of synaptic plasticity and why we need it.
Brain Plasticity
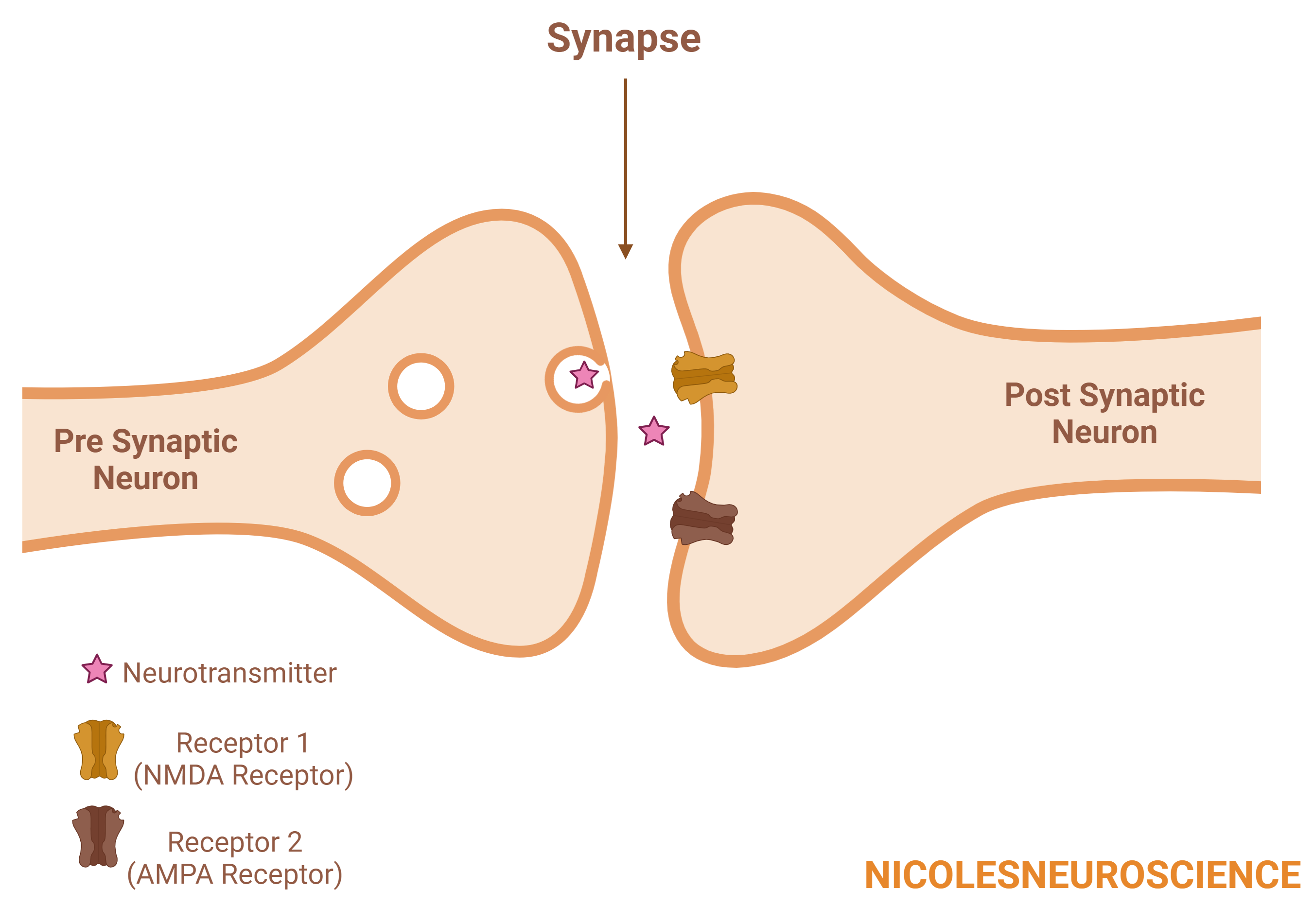
Brain plasticity is a term that describes the brain's ability to change. We can break this down further into synaptic plasticity and neural plasticity. Synaptic plasticity looks at changes at the synaptic level (the space where two neurons meet and communicate; Figure 1), while neural plasticity looks at whole network changes across multiple neurons and multiple brain areas. Synaptic plasticity is really cool in my opinion because you can literally see the space between two neurons change to accommodate a stronger signal.
Synaptic Plasticity
Synaptic plasticity means that synapses can change, and there’s essentially two ways a synapse can change. The synaptic connection can either get stronger, known as long term potentiation (LTP)1,2, or the connection can get weaker, known as long term depression (LTD)1,2. But what does a stronger synapse look like?
Long Term Potentiation – Stronger
The strength of a synapse is controlled by (1) the amount of neurotransmitters being released from the PRE synaptic neuron and (2) the amount of receptors waiting for neurotransmitters on the POST synaptic neuron1,2.

LTP is sometimes called a ‘coincidence detector’ because you need to have the presynaptic neuron releasing the neurotransmitter at the same time as the postsynaptic neuron receives the neurotransmitter.
Anyway, let’s look at what’s going on together.

What we can see here is that on the presynaptic cell, the neurotransmitter is released, which then causes receptor 1 (known as an NMDA receptor) to activate. Receptor 1 allows calcium inside the cell, which through a lot of different steps, causes receptor 2 (known as an AMPA receptor) to be brought to the synapse. So the next time the presynaptic neuron signals to the postsynaptic neuron, the postsynaptic neuron has more receptors to detect the signal, and in turn, will send a stronger signal foward1,2.
Long Term Depression – Weaker
In contrast, long term depression occurs when the presynaptic neuron releases neurotransmitter, but the postsynaptic neuron does not produce any response1,2. Although receptor 1 will still release calcium, it is at a different frequency, causing different steps to occur. Instead of receptor 2 being brought to the synapse, it is actually taken away from the synapse. Therefore, in the future, the postsynaptic neuron will respond weakly following neurotransmitter release from the presynaptic cell.

But who cares?
Well, for one, I do. And you should too, because we need LTP and LTD to store memories, learn, and establish new habits.
For one, we see LTP occurs after learning3. We also see that the reversal of learning reverses LTP4,5. We know that if we block LTP, we do not get learning6. In terms of memory, we see that new dendritic spines (imagine tiny trees coming off of neurons searching for neurotransmitters) which appear after learning are maintained over a lifetime7. This indicates that LTP is one way we store memories. Interestingly, we also see LTP in the striatum, known for dopamine and habit formation.
We also need LTP and LTD to help us recover from injuries to the brain.
We see that interventions supporting LTP and LTD, such as cranial stimulation, improve brain function in various disease areas. In Parkinson’s disease, a clinical trial showed that repetitive transcranial stimulation improved motor performance, although these benefits did not last long enough to be used long-term9. In schizophrenic patients with auditory hallucinations, slow transcranial stimulation induces LTD-like changes, leading to a decrease in auditory symptoms.
(Note: Learning is not only about strengthening connections, but also about weakening ones that are no longer important, like learning that we do not need a fear reaction when we meet someone new!)
In trying to better understand how this occurs, studies have shown that transcranial stimulation leads to BDNF production, which is critical in LTP and LTD10. The authors suggest this could have implications for stroke treatment10.
But what else controls synaptic plasticity? Can we exert any influence over it? Stay tuned for next week’s newsletter and pick up a copy of Rewire!

My Neuroscience Thesis

And here it is! My beautiful contribution to the mouse connectome project. I helped rebuild a section of the mouse somatosensory cortex in an attempt to understand how neurons communicate with one another in the mouse brain.
Using imaging techniques, we traced the individual neurons from 500 images taken from slices of a mouse brain. Once my team and I had rebuilt this (we were in a team of 6), we were tasked with looking at the interactions between excitatory and inhibitory neurons to understand the relationship between synapse size and strength and their communication with nearby dendrites.
In the brain, there is a delicate balance between excitatory neurons, which promote activity, and inhibitory neurons, which calm things down. Excitatory neurons primarily use the neurotransmitter glutamate, while inhibitory neurons often use GABA (gamma-aminobutyric acid). GABAergic neurons, which release GABA, are essential for maintaining this balance.
In epilepsy, the GABAergic system can malfunction, meaning the brain doesn’t have enough inhibition to counterbalance excitation. When excitatory activity becomes excessive and unregulated, it can lead to hyperactivity of neurons, which results in seizures. This loss of balance is critical in epilepsy because GABAergic inputs help regulate synaptic plasticity—the way neurons adapt to changes—at nearby glutamatergic synapses. Without proper GABAergic function, the overall excitatory activity in a network or dendrite becomes too high, leading to seizure activity.
I hope you enjoyed this bonus piece of information!
Until Next Week,
Nicole x
P.S. Leave a comment with any topics you want covered in future newsletters!
References
https://www.sciencedirect.com/science/article/pii/S0301008201000132
Rioult-Pedotti, M. S., Friedman, D. & Donoghue, J. P. Learning-Induced LTP in Neocortex. Science 290, 533–536 (2000).
Kim, W. B. & Cho, J. H. Encoding of discriminative fear memory by input-specific LTP in the amygdala. Neuron 95, 1129–1146.e1125 (2017).
Nabavi, S. et al. Engineering a memory with LTD and LTP. Nature 17, 348–352 (2014).
Martin, S. J., Grimwood, P. D. & Morris, R. G. M. Synaptic plasticity and memory: an evaluation of the hypothesis. Annu. Rev. Neurosci. 23, 649–711 (2000).
Yang, G., Pan, F. & Gan, W.-B. Stably maintained dendritic spines are associated with lifelong memories. Nature 462, 920–924 (2009).
Loved this week's newsletter! Especially that you had added the figures, it makes it easier to understand.
I'd love to hear more about weakened connections vs overriding connections. I've read and heard from neuroscientists (in podcast) that habits can't be weakened nor forgotten, but only overriden by a stronger connection in form of a new habit, or rather a new behaviour from the cycle cue/new behaviour/reward. But then I've also read that neural pathways can be weakened, so I'm uncertain if this then does not includes habits? From my understanding, habits are stored in the basal ganglia, has that something to do with it? I'd love to know how it's all connected (pun not intended)!
Thank you from a curious mind! :)
Hello Nicole,
Thanks for the share. I am currently reading your book and enjoying it very much. The facts provided in it does answer some questions i had and crushes (in a good manner) some stories I had been taught. Relying on facts is enlightening.
Would you know by any chance how the Enteric Nervous System is interfering with the brain in term of behaviour. I have not yet find an article yet who can explain the behaviour of a person i know who, she had her vagus nerves cut when she was a child (oesophagus was shortened to 4cm). This person doesn't seems to feel any tiredness, she is 76 today. I have seen her undernourished, sick and yet the moment her body has the littlest food she is up, running and smiling. She is a smart person. It's troubling, and I don't know if this is a common pattern in people who are in such situation as it is rare.
It seems that her behaviour is not influenced by her guts, but I am not sure of anything.
If you had any piece of information that may even give a little light, that would be helpful.
I have found this article
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7495222/#:~:text=The%20enteric%20nervous%20system%20is,functions%20of%20the%20gastrointestinal%20tract.
And a few others but it can only lead to assumptions.today i am also considering it may be a form of autism.
Thanks,
CP